
Dr Robin Bell and Professor Leo Jeffcott
Equine Performance and Imaging Centre Sydney University Veterinary Teaching Hospital Camden
In this article we will attempt to give you an overview of the problems that can affect the knee in the horse, by firstly reviewing the anatomy, the role conformation plays, and finally discussing in more detail the more common conditions that affect this joint in the horse.
Anatomy and Conformation
The horse’s knee is one of the most complex regions in the limb. This is because there are a number of small bones and ligaments all combining to form the three main joints.
These are the radiocarpal, intercarpal and carpometacarpal joints. There are 9 (and sometimes up to 11) bones that make up these knee joints. The small bones in the knee are arranged in two rows which articulate either the radius at the top of the knee, or the cannon and splints at the bottom. These bones are held together by a complex series of ligaments that help maintain joint stability but also act as shock absorbers during exercise. 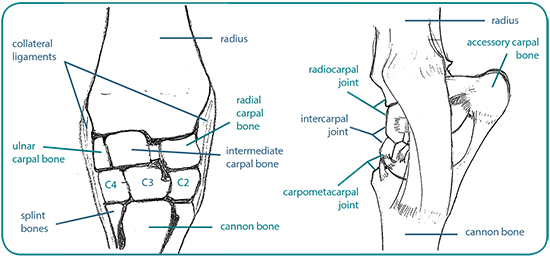
Conformation is very important in the horse’s knee. Disorders in conformation can be caused by factors encountered prior to birth such as immaturity, abnormal positioning of the foetus within the uterus, and those that occur after birth such as excessive nutrition, over-exercise and external trauma. The Functional Anatomy and Biomechanics Group at Melbourne University have spent a number of years carefully examining the conformation of the knees of racehorses, and their early results suggest that conformation plays a significant role in poor performance. Then, in addition to this, recent studies have disputed the long held belief that all deviations in the knee are detrimental. In particular a study of racing Thoroughbreds showed that turning in of the knee (varus deformity) of a few degrees was actually protective against fractures, and other studies have suggested that a deviation of up to 5 degrees should be considered normal. However, other conformational defects such as outside deviation of the knee (carpal valgus), bench knees, forward or backward deviation of the knees have been associated with an increase risk of injury and lameness.
Diagnosis
As with the other regions of the horse that we have covered previously, lameness is localised to the knee by a combination of physical examinations, examination of gait, flexion tests and nerve blocks.
Injection of local anaesthetic into the knee joints is a very effective means of localising lameness to the carpus
Generally it is relatively easy to ascertain that lameness is coming from the horse’s knee, but it is more complicated to be exact as to what is causing the problem because of the complex anatomy of the region, and the similarity in the presenting signs for these conditions. Despite recent advances in MRI, CT and Nuclear Scintigraphy, the most useful techniques remain the use of x-rays and ultrasound and with these the greatest majority of pathology affecting the knee region can be diagnosed. We will now discuss four of the most commonly encountered knee ailments in performance horses: osteoarthritis, chip fractures, proximal suspensory ligament desmitis and third carpal bone sclerosis.
Osteoarthritis of the knee joints is by far the most common condition affecting this region in horses, and it is often secondary to other problems such as chip fractures or poor conformation. There are two main categories of osteoarthritis in the horse, that seen in racehorses (or ex-racehorses) and a slightly different clinical presentation seen in older horses which is much less common. In racehorses the osteoarthritis develops secondary to stress-related changes in the bone and cartilage within the knee joints because of the stresses of training and racing. Osteoarthritis in older horses seemingly develops without the cycle of exercise-induced bone and cartilage remodelling and damage. These horses may show dramatic abnormalities on x-rays with relatively minor clinical signs. Horses with chip fractures are prone to arthritis, and some horses with chronic arthritis will develop knee chips. Horses with carpal osteoarthritis are typically lame, and will have some degree of joint swelling. They will generally have a decreased range of motion of the carpus and will be painful when the joint is flexed. Instillation of local anaesthetic into the affected carpal joint most often eliminates this lameness and helps identify the specific joint involved. Diagnosis is also aided by the use of radiographs and in more difficult cases, a bone scan can be of value. Treatment for the condition once it has developed revolves around minimising the clinical signs and relies on medications injected directly into the joint, rest, and treatment with anti-inflammatories such as phenylbutazone. In severe cases when the horse is used for breeding or kept at pasture rather than athletic performance, surgically fusing the joints with a total or partial carpal arthrodesis (joint fusion) may provide relief from lameness. Figure 3 shows the radiographic changes of a case of severe arthritis in the knee. 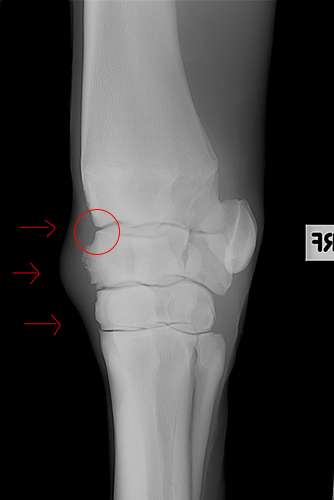
Radiograph of the knee of a 7yo Thoroughbred gelding. Notice the large amount of new bone formation (circle), and the associated joint swelling (arrows)
Carpal Chip Fractures
Properly termed ‘osteochondral fragmentation’, carpal chip fractures are primarily a disease of racing or ex-racing horses. They are caused by the same cycle of bone and cartilage damage that induces osteoarthritis, and the two conditions are often seen together, (i.e. horses with chip fractures often develop osteoarthritis, and horses with osteoarthritis can develop chip fractures). Lameness in horses with small chip fractures ranges from mild to severe, however, most horses are initially very lame. Lameness severity depends on number and location of fragments, and whether these fragments are present in both knees. Horses with this condition show heat and swelling over the carpal joint, and these horses resent flexion of the affected knee. Most carpal chip fractures are visible on x-rays, although bonescan, and more recently MRI can be very useful in the diagnosis of early chip fractures. Definitive treatment relies on surgical removal via keyhole surgery (arthroscopy), and this removal minimises the chances of significant arthritis developing in the joint.
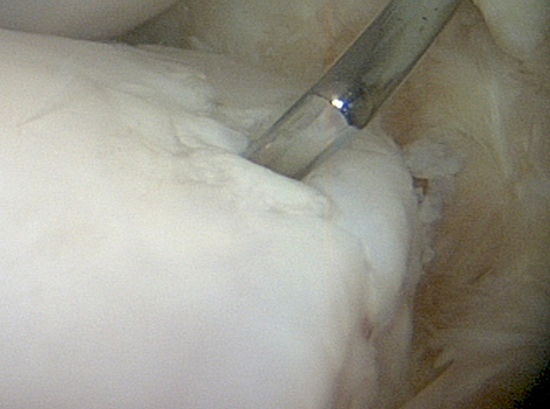 Intra-operative picture of a carpal chip fracture at arthroscopy. Note the probe being used to ascertain that the fragment is loose. Note also the roughened cartilage surfaces which should ordinarily be extremely smooth.
Intra-operative picture of a carpal chip fracture at arthroscopy. Note the probe being used to ascertain that the fragment is loose. Note also the roughened cartilage surfaces which should ordinarily be extremely smooth.
However, with small fragments in particular, the use of intra-articular medications can result in improvement in the clinical signs. In any case, whether horses are treated with surgical removal or managed conservatively, rest is an essential part of the treatment, as it allows the fracture bed, and surrounding tissues, a chance to heal. Prognosis is dependent on a number of factors, including use of the horse, age, severity of the fractures and presence of arthritis. In racing horses, approximately 70% of affected horses can be expected to return to their pre-injury level of performance, however, in horses with the most severe cartilage damage, only 50% returned to full work. Prognosis for performance horses, especially with timely removal of fragments is much better.
Proximal Suspensory Ligament Desmitis
Discussion of this condition is included due to the close location of this portion of the suspensory ligament to the knee. Additionally, depending on the technique used when performing nerve blocks, lameness caused by proximal suspensory desmitis may be alleviated when performing a middle carpal joint block or vice versa. This condition generally results in an acute lameness that may resolve within 1-2 days of rest, but returns when the horse is worked again. Lameness is generally only mild to moderate, and is often worst on soft ground with the affected limb on the outside of the circle. In horses used for eventing and dressage the condition may affect both front legs, these horses may present with a change in their gait rather than overt lameness, and often the gait abnormality is not apparent unless the horse is in medium or extended trot. In horses used for showjumping, the primary clinical sign may be a tendency to land with the unaffected limb as the lead leg. Diagnosis is made using a combination of nerve blocks to localise the lameness to the region of the suspensory ligament, and then ultrasound to provide a specific diagnosis.
In cases where ultrasound does not provide an answer, MRI or CT can be used to establish the specific diagnosis. Bone scan is indicated, particularly in cases where there is a fracture in the top of the cannon bone at the origin of the suspensory ligament. 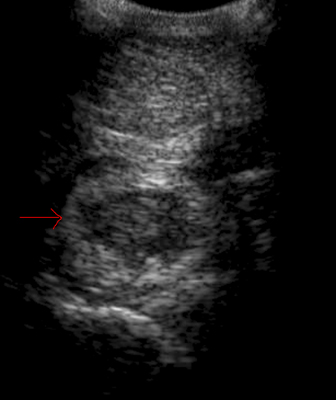
Ultrasound picture of severe suspensory ligament tear, with a large darkened core lesion (red arrow) in the body of the suspensory ligament.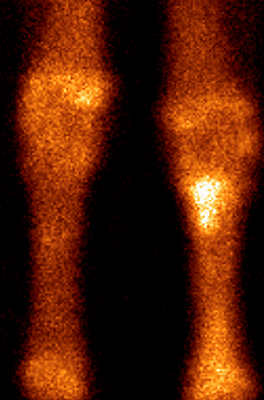
Bonescan of horse with tearing of the origin of the suspensory ligament at the origin on the cannon bone, and fracturing of the bone at this level. The bright spot in the left side of the images indicate this process.
The majority of horses are able to return to full athletic performance (between 85-90%). As with most tendon and ligament injuries, a period of confinement and rest is the cornerstone of initial therapy. After the initial 2-3 months of confinement and walking some cases benefit from the stimulation of trotting exercise once the horse has been rested for 2-3 months. Other reported treatments include shockwave therapy, injection of corticosteroids or regenerative medicine products into the origin of the ligament and surgical splitting of the origin of the ligament.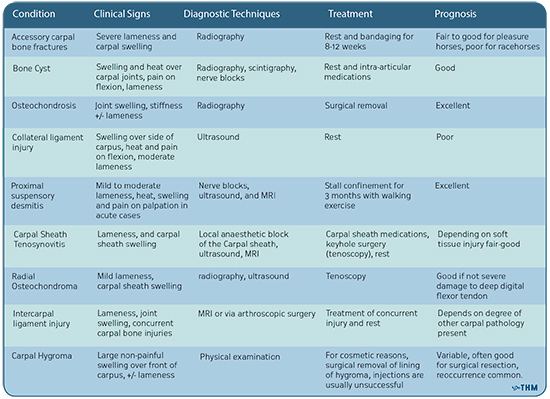 As you can see from the table above, there are many problems that can cause carpal lameness in horses, and diagnosis can sometimes be difficult. We hope that with a better understanding of the anatomy and predisposing factors, you will appreciate the complexities of managing lameness in the region, and how your vet will tackle the problem.
As you can see from the table above, there are many problems that can cause carpal lameness in horses, and diagnosis can sometimes be difficult. We hope that with a better understanding of the anatomy and predisposing factors, you will appreciate the complexities of managing lameness in the region, and how your vet will tackle the problem.
This article first appeared in the June 2012 issue of THM.
This is a very useful article; clear and easy to understand, putting perspective into the problem of lameness .
Great illustration of the knee.
Very informative read.
My horse’s knee looks exactly like that, and this is article helped me understand what is wrong with his knee.
My mare has fractured the first carpal bone off side leg she’s is mildly lame at the trot is it possible to not have surgery and just keep her for breading
Our horse has no swelling of the knee someone said it was a minsucus tear
thank you for this valuable information. It gave me some idea’s of the different things that could be wrong with his knee and what to do about it. Thank you
Our race horse has a 3rd carpal hairline fracture will he race again after 6 mths rest he is nine year old
Astonished by the ‘excellent’ prognosis for Proximal Suspensory Desmitis, my horse went on loan and returned with this and he was chronically lame and only five and a half. I joined a support group and found that most people ended up having shock wave therapy then operating and even then the return to work wasn’t guaranteed long term.
I am beating myself up for not rescuing an Appaloosa mare I recently saw at a horse sale where there were of course”Killer Buyers”. This mare was well trained and had had a few foals. She was 13 years old. She had a very obvious knee injury and swelling that went up above her knee on the outside of her leg. The injury looked healed in that there were no open wounds but the knee was still very swollen with no fur covering her knee just scar tissue. I didn’t buy her because my husband didn’t want me to but it. Broke my heart because she had knickered at me as I walked by seemingly asking me for help. PLEASE NEVER take your horse to an auction! What they have to endure before slaughter is horrific. It is much kinder to get a vet out to euthanize them even if you do have to pay a bit of money to have it done. This is much kinder than having the horse forced onto a truck loose with many other horsed and driven for miles without food or water to the slaughter house. I have been very depressed for several days over seeing this mare. I wish there could be an end to horse slaughter and that owners were more responsible and humane! I think there should be laws protecting horses from inhumane treatment during transport to the slaughter house.
P.S. I would like to add that there were about 10 older miniature horse and pony stallions at this horse sale that the owner told me he had to “get rid of” before his mares! We are in a very bad drought right now and people seem to be “dumping” horses at these sales at which I know are killer buyers. I asked a lady there if they actually load the minis onto the truck with the big horses and she told me that “I have seen them do it”. Can you imagine what would happen to these little horses during transport underneath the hooves of the big horses?!!! I can only imagine. Once again PLEASE Do NOT take your unwanted horses to a horse sale or auction with Killer buyers. If you cannot feed them because of drought or afford proper medical care such as gelding unwanted colts then be humane enough to have them euthanized by a veterinarian and STOP OVER BREEDING HORSES!!!!! 🐴🐎🏇🐴🐎🏇🐴🐎🏇🐴🐎🏇🐴🐎🏇🐴🐎🏇🐴🐎🏇🐴🐴🏇 Their are simply not enough good homes for all of them.
I agree whole heartedly with Anonymous re the awful and unnecessarily cruel treatment that horses and most other animals for slaughter are subjected to.
In general the indifference of too many humans to the suffering endured by too many other emotionally complex and relatively helpless warm blooded animals is a shameful indictment of humanity in general.
The supposed benevolence and other noble and morally righteous self serving dedcriptions of the human condition are in the main simply delusional self deceptions that ease the burden of having to admit to yet another example, where we rationalize our moral and ethical short comings so as to avoid facing and adhering to the obligatory empirical standards that decency and compassion demands!