

Professor Andrew Dart – University Veterinary Teaching Hospital
University of Sydney, Camden, NSW Australia
Most of us have experienced the unsettling sound of a roarer. Is it as distressful for the horse as it is for the rider, or the spectator? What, if anything, can the vet do? Professor Andrew Dart of the Sydney University Veterinary Hospital explains what causes the noise, what can be done to fix it, and tells us how the condition affects our horses.
The larynx acts as a valve at the back of the throat regulating airflow into the trachea and on to the lungs. There are two cartilages called the arytenoid cartilages that form the margins of the larynx. These cartilages open and close the airways under different circumstances. When a horse is swallowing the arytenoid cartilages close to prevent food from entering the trachea while, during maximum exercise, the arytenoid cartilages are wide open to allow the free flow of air into the trachea and into the lungs.
Horses can develop paralysis of one or both of the arytenoid cartilages so they no longer function. Most commonly the left arytenoid is only affected because the nerve supply to the left arytenoid is unusual in that it is an exceptionally long nerve and is more susceptible to damage. Left laryngeal paralysis can affect any breed or age of horse but is more common in bigger horses with long necks because the nerve is longer. It is most commonly recognized in Thoroughbred and Standardbred racehorses because any reduction in airflow in these breeds has a significant effect on performance. However it is also seen in dressage and eventing horses, draft horses as well as most other breeds so the incidence in the general population is likely to be higher.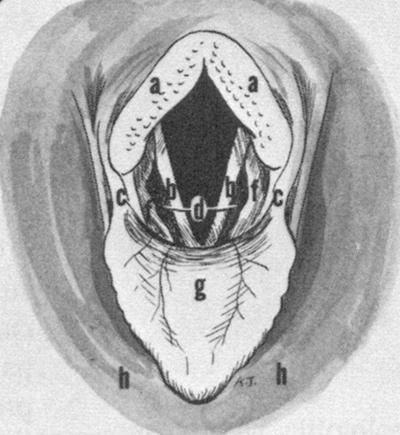
A schematic diagram of the opening of the larynx
a. corniculate processes of the arytenoid cartilages
b. vocal folds
c. aryepiglottic folds
d. laryngeal saccules
f. ventricular folds
g. epiglottis
h. soft palate
Horses with laryngeal paralysis appear clinically normal at rest. With exercise they may be heard to make a “roaring” noise, hence horses with this condition are commonly called roarers. The disease seems to only have a significant effect on performance in horses at maximum exercise. At maximum exercise, as the demand for oxygen increases, the forces generated by the horse breathing create a negative pressure in the trachea. This negative pressure gradually sucks the paralysed left side of the larynx across the airway, significantly narrowing the opening. When we visualise the larynx in horses at racing speeds on the treadmill, performance progressively diminishes as the left arytenoid moves from a neutral position and is sucked across the airway.
Horses with this left arytenoid paralysis can usually perform comfortably undertaking less strenuous activity but often make a noise. Horses at elite levels in dressage and eventing usually present for surgical correction of the problem because the noise they make is causing concern rather than for exercise problems.
Diagnosis
Left laryngeal function is commonly divided into four grades. The grade of paralysis influences how easily the condition can be diagnosed.
Grade 4 is complete paralysis. This can be diagnosed on endoscopic examination (a small camera is placed in the nostril of the horse) of the standing horse at rest. There is no movement of the left arytenoid.
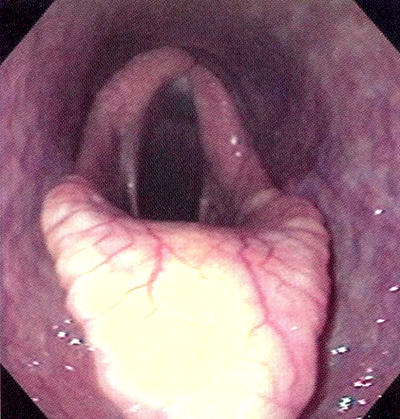
A grade 4 paralysis of the left arytenoid cartilage seen through an endoscope in a standing horse. There is no movement of the left corniculate process while the right side is in a normal semi-open position.
Grade 3 is asynchronous movement of the left side compared to the right, however the left arytenoid is unable to completely open. In most cases horses with grade 3 paralysis will develop complete collapse of the arytenoid under exercise conditions. So horses with Grade 3 and 4 laryngeal paralysis can be diagnosed at rest and do not need to be put on a treadmill to complete the diagnosis.
Grade 2 corresponds to asynchrynous movement of the left and right arytenoids at rest but the left arytenoid can fully open. Some of these horses will progress to complete paralysis during work so need to be diagnosed with the endoscope fixed in the airway and under exercise conditions, usually on the treadmill.
Grade 1 is normal synchronous movement with full abduction.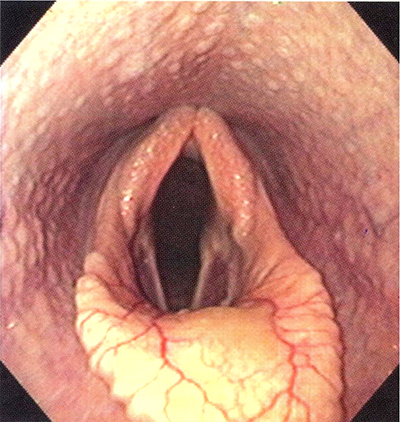
The appearance of the opening of the larynx of a normal (grade 1) airway through a videonendoscope.
Because we suspect that laryngeal paralysis is associated with a progressive degeneration of the nerve it is very likely that horses with signs of being a Grade 2 or 3 roarer will progress with time to complete paralysis (Grade 4).
Recently a new videonendoscope has become available which allows horses to be examined when exercising on the track rather than the need for endoscopic evaluation on the treadmill. The accuracy of this approach in diagnosing upper airway conditions remains to be established. Until comparative studies are performed, examination on the treadmill currently remains the gold standard for diagnosis of dynamic upper airway disease.
Treatment
There are two current approaches to treatment. The most common approach is to surgically suture the arytenoid into a semi-open position. This is the most commonly performed procedure. The alternative technique involves the implantation of a nerve into the paralysed muscles to try and re-engage activity. This nerve is transplanted from another muscle so it fires when the horse exercises; this technique would be more widely accepted if results were more predictable. In experimental cases where the nerve is surgically cut to provide a model for the disease the technique reportedly works well. However in clinical cases where horses present with a paralysed muscle there is shrinking of the muscle and fibrosis, which leads to long convalescence period and variability in outcome.
The more traditional suture technique dates back to 1970 and the principle of the procedure remains largely unchanged. However, over the years a variety of suture materials have been used and the number and the position of the sutures may vary from surgeon to surgeon. There has been little or no research investigating the optimal suture number or position. Ultimately, the aim of the procedure is to place a suture in the larynx in the direction of the paralysed muscle to optimise the area of the airway. Recently it has been discovered that the affected muscle is made up of two muscle groups responsible for opening the larynx. These muscle groups pull on the arytenoid in different directions to open the larynx or airway. The lateral muscle group has been shown to play a greater role in elevating the arytenoid cartilage and opening it more laterally while the medial muscles group produces rotates the rim of the cartilage into a more open position. Obviously these observations may have direct implications on the optimal position of the sutures.
In a recent series of studies we investigated the optimal position and number of sutures to maximise the opening of the airway. Specifically, to investigate if alternate or additional suture placement could result in more rotation of the arytenoid cartilage and greater cross-sectional area of the airway. In addition to position, the tension placed on the suture will affect the area of the airway. Excessive tension may lead to the suture pulling though and failure with subsequent loss of airway diameter. Younger horses with softer cartilage in the larynx are suggested to be more likely to suffer suture failure and it has been suggested that less force is needed on the suture to open the airway because the cartilage is more flexible.
In our first study we found two sutures – one placed along the midline and one slightly lateral to it – provided the optimal suture configuration and resulted in a greater cross-sectional area of the rima glottidis than with either suture alone. The actions of these two sutures were similar to the action of the lateral muscle group. In this study the suture tension was not quantified.
We then added another suture that ran parallel to the medial muscle group to see if this would further open the airway. In this study we found that beyond 20 newtons of tension on any individual suture there was no increase in the diameter of the airway and that the optimal tension on the suture is likely to be 15 newtons. But the study established that two sutures placed parallel to the line of action of the lateral muscle group and tied to 15 newtons provided the optimal airway.
The final study was undertaken to determine the effect of the age of the horse on the tension required to fix the airway in an optimal position. This study found that with increasing age the airway did not open as far when the same tension was placed on the suture, however the effect was not clinically significant. Most horses presenting with paralysis of the left arytenoid are young horses although the study suggests there is no need to tie the sutures tighter in the case of older horses.
Outcome
It is important to realise that fixing the paralysed arytenoid with a suture in a semi-open position will not bring the airway back to normal function. It is to be anticipated that there will be some reduction in airflow. However, it is impossible to know what this translates to in loss of performance. We do know that a loss of performance on the treadmill is seen clinically as the paralysed arytenoid is sucked across the airway significantly narrowing the airway opening and minimising oxygen flow to the lungs. However, the horse appears to cope well with a reduced airway before the paralysed airway is sucked across, at least over shorter distances. We also know that after this surgery elite athletes can go back and perform well. It is generally accepted that by fixing the paralysed arytenoid with a suture, horses with ability can go back and perform at an elite level. For Thoroughbreds and Standardbreds the aim is to optimise the airway diameter whereas for other sport horses fixing the arytenoid will minimise the noise made during work and is the aim of the surgery. Some noise particularly at maximum performance may still occur after this operation.
One complication reported is aspiration of food into the airway. Because the larynx is tied partially open it is possible food can fall into the airway when horses swallow. This risk can be reduced by taking the horse to a specialist equine surgeon experienced in performing this procedure. Note the food around both nostrils as it drains from the airway.
Complications of this surgery can include aspiration of feed into the airway. By tying back the arytenoid into a fixed position it is possible food and water may enter the airway during eating and drinking. It is not uncommon to see water flow from the nose when these horses drink after this surgery but this rarely causes a problem. This risk can be minimised but not completely eradicated by using the two suture technique and optimising the placement of the sutures. If persistent aspiration does occur the surgery is generally considered unsuccessful. This complication can be minimised by taking the horse to a specialist equine surgeon who is experienced in this technique. Nonetheless, aspiration is always a risk of surgery. The suture can be removed to reverse the effect if it is apparent soon after surgery, however if suture removal is delayed then aspiration will be permanent. Other complications include infection of the suture and failure or pull through of the suture. There is some evidence to suggest that horses with laryngeal paralysis returning to the elite performance level may be at greater risk of bleeding into the lungs.
Summary
These recent studies have optimised the technique for surgical correction of left laryngeal paralysis. Horses are often not diagnosed with this condition until early in their performance career. While sport horses can perform comfortably with this condition, the noise associated with work often leads owners to corrective surgery. In these cases surgery offers a good prognosis because fixing the arytenoid without over-tightening the suture will dramatically decrease any noise and minimise complications. The aim of surgery is to fix the paralysed arytenoid in the most open position without creating aspiration of feed as a complication. There is more and more evidence that the aim should be to fix the arytenoid so it is not sucked into the airway during work. The two suture technique seems to provide the optimum airway and provide back up should one suture pull through. Optimal suture placement may also reduce the risk of aspiration by contouring the paralysed arytenoid into a shape that minimises risk of aspiration. This is a procedure that should be performed by an experienced equine surgeon, but even under optimal conditions the risk of complications that may end the performance career of the horse should be considered before proceeding.
Can this be a sequela to CNS nerve damage as a result of EPM?
Can horses recover from this